Inclusivity in medical education: a step forward and tools that can help
By Roel Smabers, Robert Smeenk & Britt Bomhof
In recent years, there has been a justified increase in attention to inclusivity within medical education. A diverse student population and an inclusive learning environment are essential for training doctors who can effectively deal with a diverse patient population (1,3). About 20 years ago, the physician population was predominantly male and white. Since then, significant progress has been made in the ratio of men to women. Among all doctors, the number of women has grown from 32% in 2005 to 46% in 2016. In 2016, there were not yet more female doctors than male, but now there are across all doctors. Among specialists, the increase was from 26% in 2004 to 41% in 2016. The percentages vary considerably within specialties: cardiac surgeons and orthopedists were still predominantly men in 2016, at 11% and 12% respectively. And this ratio has not changed much yet.
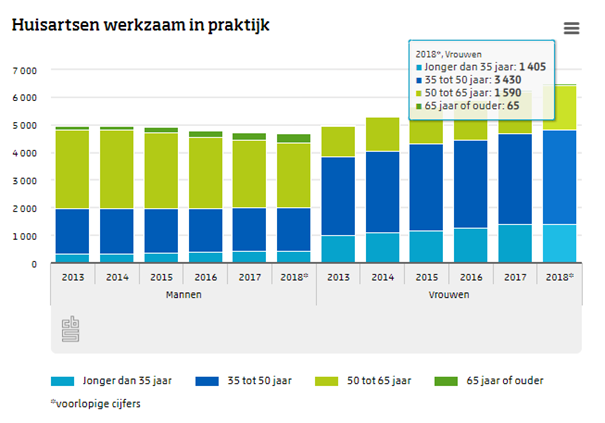
Among general practitioners, this is the case, according to (Dutch) figures from the CBS. We see that the number of female GPs is now greater than the number of male GPs.
Although considerable steps have been taken in the ratio between men and women, there is still much room for improvement. Currently, the number of medical specialists with a migration background is estimated to be between 2 and 4 percent.There is still much work to be done if the physician population is to become a reflection of our society. This work begins in the training programs. And although we should not overestimate the contribution and role that digital systems can play in this, we do think that a portfolio tool can help. In this article, we explore the current state of affairs and how digital tools such as e-portfolios can contribute to more inclusive medical education.

The challenges of inclusivity in medical education
At the 2024 conference of the NVMO (Dutch Association of Medical Education) with the theme ‘Equal Opportunities in Healthcare Education’, inclusivity was the main theme of the conference with a full program line on this topic. This shows that there is certainly attention to the subject within education. Yet much research also shows that inequality still exists in access to medical education. Students from affluent families or with parents in the medical sector have a greater chance of being admitted, while students with a migration background are underrepresented (3). This lack of diversity not only has consequences for the students themselves but also for the quality of healthcare as a whole.
In addition to the selection procedures, experiences during the training also pose a challenge. Students from minority groups regularly report experiences with aggressions and subtle forms of discrimination (3). These experiences can have a negative impact on their well-being and performance.
Towards a more inclusive curriculum
Research worldwide also shows that diversity within medicine improves its quality. And when we see that there is still a considerable imbalance between the physician population and society, there is still a lot to be gained.One of the studies recently conducted at the GP training programs has formulated a so-called DEI (Diversity, Equity, and Inclusivity) strategy. This consists of 7 very concrete strategies, of which these are the most important:
- DEI expertise promotion for all those involved in GP training using training programs;
- Appointment of DEI ambassadors in all teams of GP training, who contribute to knowledge transfer, reflection on possible prejudices;
- Participation in DEI networks; Giving an active voice to trainees from ethnic minority groups in developments within GP training.
Despite the fact that there is a lot of attention and a number of initiatives have already been started within medicine, there are still plenty of challenges remaining. To address these challenges, it is essential that medical education actively works towards a more inclusive curriculum. In general, the following aspects are often mentioned as supporting the process towards more ‘DEI’:
- Awareness of implicit biases
- Knowledge about health issues specific to particular groups
- Skills to communicate effectively with a diverse patient population
The role of digital tools in inclusivity
Digital tools, including e-portfolios, can make a modest but potentially valuable contribution to promoting inclusivity in medical education. For example, we see in studies on biasing and the transfer of graduated doctors to the practical work environment as residents (learner handovers), the influence of negative feedback has a major impact on how the learner continues the learning path. A student who carries negative feedback consistently receives lower grades. And often this happens unconsciously or at least out of sight.
A number of very practical tools to promote diversity are:
- Personalized learning: E-portfolios allow students to follow their own learning path and reflect on their experiences. This can help recognize and value the unique perspectives and backgrounds of students.
- Equal opportunities for feedback: Digital platforms can provide a more structured and objective way of giving feedback, reducing the chance of unconscious biases.
- Accessibility: Online tools can increase the accessibility of education for students with physical limitations or other challenges.
- Cultural competence: E-portfolios can contain specific modules aimed at developing cultural competence, better preparing students to work with diverse patient populations.
Conclusion
Although digital tools such as e-portfolios may contribute more positively to more inclusive medical education than we think, they are only part of the solution. Real change requires a holistic approach, where all aspects of the training are critically examined and adjusted. Instruments or concepts such as ‘workplace-based assessment’, programmatic assessment, multi-source feedback, OSCE, where the origin of a decision can always be clear for the learner and the assessor, can be very useful in this regard. That’s why we believe these are also important elements of a good digital portfolio. Especially now that algorithms and AI support are increasingly being applied in such tools.
Creating an inclusive learning environment in medical education is not only a matter of justice for students but also an investment in better healthcare for everyone. By embracing diversity and promoting inclusivity, we train doctors who are better able to provide care to an increasingly diverse society.
Sources
- https://www.huisartsopleiding.nl/kwaliteit-innovatie/opleidingsinnovatie/bevorderen-van-diversiteit-inclusie-en-gelijke-kansen-tijdens-de-opleiding/
- https://www.revalidatie.nl/ntr/diversiteit-en-inclusie-in-de-opleiding-tot-revalidatiearts/
- https://dejongedokter.nl/djd-schrijft/hoe-ver-zijn-we-al-diversiteit-en-inclusie-in-het-medisch-onderwijs/
- Naar een inclusieve opleiding in de zorg: Diversiteit en inclusie onder artsen (Obihara & Maarse 2024)
- Lee HW, Kim E. Workforce diversity and firm performance: Relational coordination as a mediator and structural empowerment and multisource feedback as moderators. Hum Resour Manage. 2019;1–19